By Bert Hoebee, Veteran
Originally published in Camaraderie 51(3) November 2020. Views and opinions expressed are those of the author and not necessarily those of DFWA.
Introduction
It is a fact that military service can lead to hearing loss in varying degrees of severity. While everything possible is done in training to prevent such injury, that is totally impossible during active service.
Since the First World War provision has been made for our servicepeople and Veterans to be treated and supported to deal with illness or injury due to their service. However, judging by the clamour of dissatisfaction, something seems to have gone seriously amiss for eligible Veterans dealing with compensable hearing loss. The support process has not worked efficiently or effectively, leaving eligible Veterans frustrated, and Audiologists equally frustrated at not being able to provide those individuals with the best possible outcome to meet their needs.
Following an examination of a number of cases where the ‘fully subsidised’ hearing aids provided under Hearing Services Program (HSP) have proven not to meet Veterans’ needs, some common factors emerge.
In this article I will examine these and possible reasons for dissatisfaction. It will conclude with a suggestion as to what affected eligible Veterans themselves can do about it.
The Factors Involved
Seven factors are involved: The unique nature of military service, Legislation, the Department of Veterans’ Affairs, the Department of Health, the nature of ‘fully subsidised’ hearing aids, Audiologists and most importantly, individual Veterans.
The Unique Nature of Military Service
The unique nature of military service and the sacrifice demanded of those who commit to defend our Nation are recognised and acknowledged by the Commonwealth. [i] With that recognition comes a commitment to support Veterans in dealing with and overcoming the physical, mental and other consequences of their service.
Hearing injuries are a frequent consequence of military service. These ‘exceptional circumstances’ compensable injuries are endemic and result from both training for war, and from operational service. It is the nature of things in warfare and in training that military personnel will be exposed frequently to loud, harsh or deafening noise. In operations that is inevitable if the military is to achieve the mission it is given. This demand on soldiers, sailors and airmen and women leads often to hearing injury recognised under the Veterans’ Entitlements Act 1986 (VEA) and requiring support. [ii]
Legislation, Policy and Process
The Veterans’ Entitlements Act 1986 (VEA) provides for treatment and support services for Veterans. Sect 80, deals with ‘treatment’ and speaks to restoring or maintaining physical and mental health, ensuring a person’s social well-being and the supply of appropriate aids and appliances. Sect 85 establishes where eligibility for treatment arises. Sect 90 (1) and (4) deal with the making of determinations that describe circumstances and conditions under which treatment of particular kinds can be provided.
Made under Sect 90 of the VEA, the Treatment Principles (TP),[iii] Sect 11.5. deals with hearing aids and Sect 11.5.4 provides that the Commission may accept financial responsibility for the supply of a hearing aid from an audiology provider if the hearing aid is unable to be supplied to the eligible person under the HSP. Note that this is subject to prior approval from DVA. [iv] Note also, that if HSP cannot provide for the needs of a Veteran, it is DVA – the Commission – that should fund them.
The Australian Veterans’ Recognition (Putting Veterans and their Families First) Act 2019, commits to beneficial interpretation and application of legislation for Veterans. It recognises that Veterans can require support mechanisms to enjoy good health, to access employment and training opportunities, to access appropriate housing, to have access to justice, to enjoy social wellbeing or to participate in community engagement.
This legislative framework establishes the basis upon which an eligible Veteran is able to obtain support in the most effective way, without undue bureaucratic obstacles being put in their way – in this case, particularly where HSP provided ‘basic’ support is not suitable to meet their compensable hearing and lifestyle needs. On the facts, DVA could be trying to abrogate or shirk this responsibility.
Department of Veterans Affairs (DVA)
DVA Portfolio Budget Statements 2019-20, speak to maintaining and enhancing the financial well-being, self-sufficiency and physical well-being and quality of life of eligible persons. The Productivity Commission [v] reinforced this objective; speaking of an overarching objective to improve wellbeing for Veterans and their families through a whole-of-life approach to restore injured and ill Veterans, provide timely and effective rehabilitation and health care to enable participation in work and life and to enable opportunities for social integration.
Complaints about the provision of hearing services to Veterans seem to suggest that DVA staff are losing sight of the Department’s overarching obligations to Veterans under the VEA. The lack of clarity surrounding the prior approval process most often leads to difficulties – many due to the ‘red tape’ nature of the bureaucratic process involved.
A particular confusion certainly seems to reign over the technology of the hearing aids supplied under the HSP’s voucher-driven process. Brochures [vi], booklets and notices [vii] are routinely re-issued and amended, and at least one Notice issued to Audiologists is incorrect in stating that DVA will not give prior approval for other than the basic ‘fully subsidised’ HSP supplied devices. That is contrary to the legislation under the VEA. Is it possible that Customer Service Officers, or the DVA Audiology Advisor are not fully aware or committed to the need to act in a way that is beneficial and empathic with eligible Veterans’ hearing and lifestyle needs arising from compensable hearing injury?
DVA’s initial reflex response for requests for approval for the Commission to accept financial responsibility under the Treatment Principles, appears often to be negative – 87% denied between July 2019 and February 2020. [viii] This negativity is often by way of a refusal along the lines of an assertion that the HSP ‘fully subsidised’ hearing aids can meet the Veteran’s needs, especially in cases where ‘prior approval’ was not sought. However, even where an Audiologist’s professional clinical analysis is to the contrary, the same assertion is made, or extensive further information is sought. Notable is the inference that ‘fully subsidised’ HSP devices must be considered, even though these only provide for ‘basic’ needs. That leads to anger and frustration on the part of Veterans, and Audiologists. It could even be taken as impugning the latter’s professional ability and standards.
Department of Health (DOH)
The DOH administers the Hearing Services Administration Act 1997. The HSP provides fully and partially subsidised hearing devices to eligible Australians who are ‘hard of hearing’ to manage hearing loss and improve community engagement – delivered through a voucher system. The HSP is resource limited, and is not charged with funding particular compensable needs of eligible Veterans, beyond basic ‘fully subsidised’ devices that it provides to the wider community. It is quite incongruous with the recognition of the unique nature of military service, for the HSP to have the support of Veterans foist upon it. Neither the HSP, nor individual Audiologists have any imperative or legislated obligation to provide beneficial and veteran centric support to eligible Veterans, despite the existence of the exceptional circumstances HSP process for Veterans [ix] that specifically fits with TP 11.5.4.
Nature of ‘fully subsidised’ and ‘top-up’ hearing aids
The HSP can provide ‘fully subsidised’ hearing aids to eligible Veterans. All such devices are of the ‘basic’ variety, which cover only the following situations: Quiet Conversations, Watching TV and Phone Calls. [x] Veterans have no issue in cases where these meet their clinically established needs.
Other, more technologically advanced aids are ‘partially subsidised’ under the HSP, and are also referred to by DVA as ‘top-up’ devices. These go in order of increasing capabilities beyond the ‘basic’ capabilities and range from Level 1 to Level 7. They can be recommended by Audiologists according to clinically determined hearing and lifestyle needs, which the basic devices are incapable of meeting for any particular Veteran. See Figure 1: Technology to suit your lifestyle.
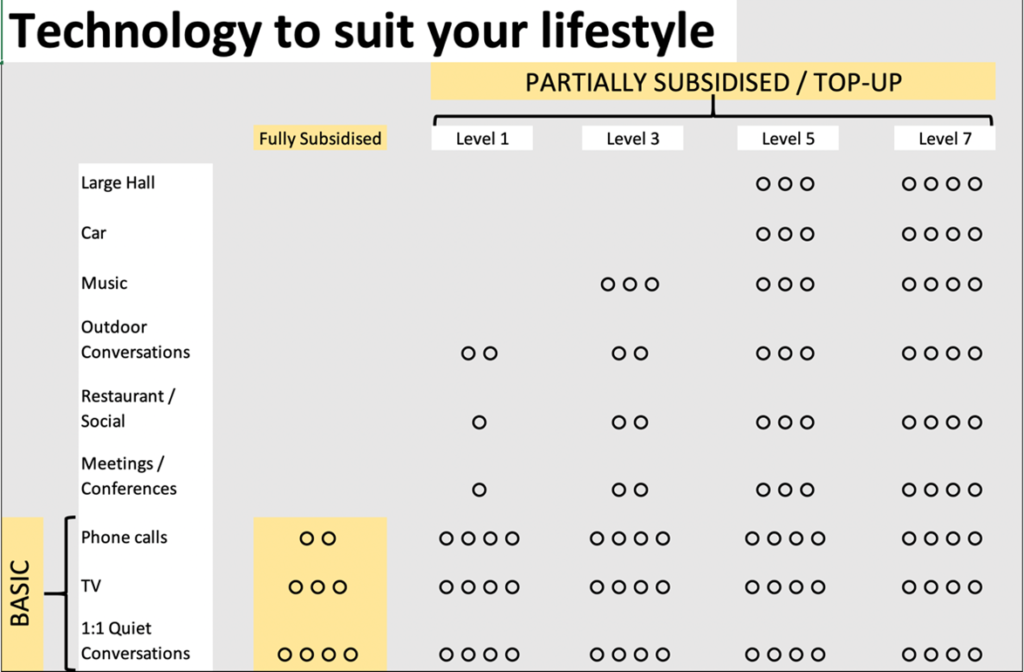
Source: Adapted from Hearing Australia, 2017 (My highlighting and annotations)
If a basic device cannot provide satisfactory capability for conferences or meetings, outdoor conversations, social and restaurant or in-car conversations, then the Audiologist is likely to recommend an appropriate device from the more capable range. A Veteran’s needs for social wellbeing and participation in community engagement could require a higher level of hearing support. However, the DVA ‘prior approval’ process must be followed.
Audiologists
Not all Audiologists appear to be aware of Veterans’ eligibilities to ‘exceptional circumstances’ hearing support services from DVA for those with needs beyond the ‘fully subsidised’ devices available through the HSP. No wonder then that Audiologists react in frustrated and less than helpful ways to requests for clinical reports to be provided to DVA to support a ‘prior approval’ request.
Audiologists might be directed from ‘on high’ and by notices such as that referred to, to not make exceptional circumstances requests to DVA or provide such reports. They might also have direction to advise Veterans with higher level needs that DVA will not approve them. It is this dysfunction (confusion, misinformation, lack of knowledge), apparently stemming from both DVA and DOH, which so angers eligible Veterans and frustrates Audiologists.
This can result in Veterans needlessly (and wastefully) accepting unsatisfactory HSP ‘fully subsidised’ hearing aids or paying from their own pocket for ‘partially subsidised’ devices, without prior approval. Most commonly, they then seek reimbursement or embark on a very long process of trying to seek prior approval. None of this is beneficial, efficient or effective in meeting the eligible Veteran’s exceptional needs in a timely manner. Lack of clarity for Audiology professionals is not in the interests of the Veterans they support.
To their credit, some individual professionally qualified Audiologists, having clinically analysed a Veteran’s hearing and lifestyle needs, are still prepared to furnish the reports that DVA calls for when approval is being sought, only to have the request ‘knocked back’, or more information being sought from them.
Such rejections suggest that Audiologists need to be more aware of what DVA wants from their clinical reports and recommendations, before those are submitted, by ensuring that every possible quibble is pre-empted in their clinical reports and that these reports recognise the exceptional circumstances that lead to Veterans’ hearing injuries (indicated and recognised in part by the relevant White or Gold Card). They should NOT be deterred from doing so, as now seems to be the case.
Where a ‘top up’ more capable higher technology device is clinically indicated, then this will need strong professional audiology support and proof to:
a. establish the full clinical hearing and lifestyle needs of the Veteran;
b. prove that no HSP device can meet those exceptional circumstances needs; and
c. identify clearly which ‘top up’ device best meets those needs.
One Audiologist suggested use of the relevant Comcare form [xi] or something similar. I consider that to be a good idea that could be put to DVA by ESOs. Issued to Audiologists with clear guidance, these could make it much easier for them to submit consistent and accurate information to support a clinical decision that ‘top-up’ devices should be provided. The DVA provided questions form [xii] should also be used.
Individual Veterans
Not all Veterans are fully conversant with their eligibility to hearing support services, including those that could run beyond the ‘fully subsidised’ devices available through the HSP. Even when they are, they might then face the obstacles put in the way of Audiologists when attempting to obtain prior approval for the supply of ‘top up’ devices. This is where most cases I have seen seem to have come a cropper – prior approval has not been sought for a variety of reasons, including lack of, or mis-information. That has led to a considerable degree of frustration and anger, needless expense, or eligible Veterans going without proper hearing support. All of that is contrary to the spirit and intent of the overriding legislated provisions for eligible Veterans.
With clear knowledge of the legislative framework for hearing services, individuals should be able to confidently proceed to having their clinical hearing and lifestyle needs met by, and with the help of, their chosen Audiologist. No eligible Veteran should need to do without, or pay for the support services they need to ensure their social well-being and the supply of aids and appliances appropriate to their condition.
Veterans must insist on the ‘prior approval’ process (where required), and convince Audiologists that the fallacy that DVA ‘will not approve’, has to be ignored. If they have the Veterans’ exceptional circumstances and interests at heart Audiologists must make a strong professional report and recommendation. This is hard for all individuals to convince them to do.
Conclusion
Hearing loss arising from serious, but totally unavoidable noise exposure during their service is an endemic injury among the Veteran community. Treatment and support for Veterans whose hearing and lifestyle needs can be met by the basic ‘fully subsidised’ aids available under the HSP are readily available, provided they obtain their doctor’s certificate and a Voucher under the HSP.
The process involved for an eligible Veteran to obtain treatment and support for their exceptional circumstances and compensable hearing loss needs, beyond basic aids, is rigidly bureaucratic, not Veteran centric and is not administered in a manner that is beneficial to the Veteran.
While ESOs might well address this issue at the policy and even political level, the ball is mainly in the individual Veteran’s court, assisted by professional Audiologists showing genuine empathy with their exceptional circumstances, and understanding their eligibility.
Veterans whose hearing and lifestyle needs go beyond those provided for by ‘fully subsidised’ devices must (themselves or with their advocate) get their Audiologist to obtain ‘prior approval’ for exceptional circumstances support from DVA under Treatment Principle 11.5.4. Particular care is required in their approach to this process. Audiologists need to be fully and correctly informed about the unique eligibility of Veterans to treatment and support under the VEA. They need to ensure that requests for prior approval, where needed, meet all of DVA’s requirements. DVA and the HSP need to collaborate to ensure that there is no doubt about eligible Veterans’ entitlements to hearing services and that the process to meet them is accurately and consistently articulated to Audiologists.
I say again, “How’s your hearing, cobber?”
Author’s post script:
Following completion of this article, a Review of the HSP was announced by the Hon Mark Coulton MP, Minister for Regional Health, Regional Communications and Local Government. See: https://www.health.gov.au/news/hearing-services-program-review
The Panel for this Review will be in place until June 2021. DVA will be making a submission, and I urge all those who have experience with support under the HSP, as eligible Veterans with recognised hearing issues, to make a personal submission to this Review.
Bert Hoebee
NOTES
[i] Australian Veterans’ Recognition (Putting Veterans and their Families First) Act 2019, General Recognition,
Sect 5 and 7
[ii] Recognition of Veterans’ injuries or illness is also possible under MRCA/DRCA.
[iii] Determination Instrument 2013 No. R52
[iv] ‘May’ is interpreted as expressing permission or sanction, or to be allowed to do something. [Shorter Oxford Dictionary, Oxford University Press, 1978]. In other words, if the HSP cannot satisfy a Veteran’s hearing and lifestyle needs, the Commission ought to / must accept financial responsibility for supply from the provider – it cannot refuse to do so.
[v] Productivity Commission Inquiry Report: ‘A Better Way to Support Veterans’, 4 July 2019
[vi] For example, HSV22, which states: “Neither DVA nor the OHS will reimburse you the additional cost in purchasing a partially subsidised hearing device or the extra cost of your maintenance agreement.”
[vii] For example, the HSP – DVA Notice to Audiologists which states that a Veteran will not be reimbursed by DVA for costs of ‘top-up’ devices.
[viii] Senate question on Notice N0 1174 given on 3 February 2020. DVA evidence revealed there were 115 requests and 15 approvals (13%) between 1 July 2019 and 1 February 2020, and asserted that: “For each of the declined requests [87%], the clinical evidence did not support the need for a partially subsidised device. In each case the treating audiologist has been asked to consider the full range of devices and services available through the HSP or to provide further clinical evidence to support the need for a partially subsided device.”
[ix] See http://www.hearingservices.gov.au About the Program – Client Information – Veteran Specific Information – Hearing Services
[x] As advised on 12 February 2020 by the Director, Hearing Program Management, Department of Health.
[xi] https://www.comcare.gov.au/about/forms-publications/documents/forms/claims/hearing-aid-request-form.pdf
[xii] The DVA booklet The veteran’s guide to better hearing, P04129, page 3-6 QUESTIONS